
Original Article |
BPESP as an ergonomic management tool: technical and legal evidence in industrial environments
BPESP como herramienta de gestión ergonómica: evidencia técnica y jurídica en entornos industrials
Felipe,
Larez1 ![]()
![]() ;
Yéssika, Maribao2
;
Yéssika, Maribao2 ![]()
(1) Carlisle Construction Materials, Carlisle, EE UU.
(2) Anglo Latin Culture 369 Research Center, Florida, USA.
Abstract
The gaps between the identification of ergonomic hazards and their technical approach in industrial environments proposes a comprehensive methodology called Business Plan Ergonomic Safety Program (BPESP). Through practical experience in 13 plants in the manufacturing sector, qualitative and quantitative improvements in ergonomic management are evidenced, including the reduction of musculoskeletal incidents, the strengthening of the preventive culture and the active participation of workers and supervisors. The methodological approach is complemented by a legal analysis of the US framework, where ergonomics is indirectly regulated by the General Duty Clause of the OSH Act. Federal jurisprudence, along with technical opinions from agencies such as OSHA and NIOSH, supports the requirement to implement ergonomic controls in the face of foreseeable risks. In this framework, the rigorous handling of compliance evidence acquires a central role, not only as proof of operational diligence, but as a key element for legal defense and the validation of preventive standards. From management, the need to integrate ergonomics into operational planning, justify technical-economic measures and comply with international standards such as ISO 45001 is emphasized. Ergonomics is not only a preventive practice, but also a legal and strategic imperative to improve productivity, reduce legal risks and strengthen workplace well-being.
Keywords: BPESP, ergonomic management, technical evidence, legal evidence, industrial environments.
Resumen
Las brechas existentes entre la identificación de peligros ergonómicos y su abordaje técnico en entornos industriales, proponiendo una metodología integral denominada Business Plan Ergonomic Safety Program (BPESP). A través de la experiencia práctica en 13 plantas del sector sector de manufacturas, se evidencian mejoras cualitativas y cuantitativas en la gestión ergonómica, incluyendo la reducción de incidencias musculoesqueléticas, el fortalecimiento de la cultura preventiva y la participación activa de trabajadores y supervisores. El enfoque metodológico se complementa con un análisis legal del marco estadounidense, donde la ergonomía se regula indirectamente mediante la General Duty Clause de la OSH Act. La jurisprudencia federal, junto con los dictámenes técnicos de organismos como OSHA y NIOSH, respalda la exigibilidad de implementar controles ergonómicos ante riesgos previsibles. En este marco, el manejo riguroso de evidencias de cumplimiento adquiere un papel central, no solo como prueba de diligencia operativa, sino como elemento clave para la defensa jurídica y la validación de estándares preventivos. Desde la gerencia, se enfatiza la necesidad de integrar la ergonomía en la planificación operativa, justificar medidas técnico-económicas y cumplir con estándares internacionales como ISO 45001. La ergonomía no solo representa una práctica preventiva, sino un imperativo jurídico y estratégico para mejorar la productividad, reducir riesgos legales y fortalecer el bienestar laboral.
Palabras clave: BPESP, gestión ergonómica, evidencia técnica, evidencia jurídica, entornos industriales.
|
Recibido/Received |
01-10-2025 |
Aprobado/Approved |
14-11-2025 |
Publicado/Published |
16-11-2025 |
Introduction
In today's industry, marked by automation, digitalization and the growing pressure for operational efficiency, ergonomics has emerged as an essential component to ensure the sustainability of production processes, the protection of occupational health, and regulatory compliance. However, despite its theoretical recognition, significant gaps persist between the identification of ergonomic risks and their technical and organizational approach, which reveals a structural disconnect between diagnosis and preventive action. These gaps not only compromise the effectiveness of occupational health and safety programs but also generate negative impacts on productivity, the work environment, and the legal responsibility of companies, especially in sectors with high exposure to physical and postural risk factors (Bazaluk et al., 2023; Fan et al., 2022).
The limited understanding of ergonomics as an applied scientific discipline, both at the operational and managerial levels, has contributed to fragmented institutional responses that are often limited to palliative measures without a technical basis, such as the reassignment of light tasks or the delivery of equipment without redesign of the workplace (Ngajilo & Ivanov, 2024). This superficial approach perpetuates inadequate working conditions that favor the development of musculoskeletal disorders (MSDs), absenteeism from work, and exposure to litigation for regulatory noncompliance (NIOSH, n.d.; Hulshof et al., 2021). Added to this is the exclusion of ergonomics in vocational and technical training programs, which has led to an excessive reliance on external consultants and a low institutional capacity to integrate ergonomic criteria into operational planning (Yunus et al., 2021). This academic omission limits the autonomy of organizations and perpetuates a cycle of structural vulnerability, especially in small and medium-sized enterprises.
The consequences of this ergonomic deficiency are manifested in multiple dimensions. From an economic point of view, the costs associated with work injuries, staff turnover, and decreased productivity are significant. In the legal field, failure to comply with ergonomic standards can lead to sanctions, litigation, and loss of institutional reputation, as evidenced by emblematic cases before the Occupational Safety and Health Review Commission (1993, 1997). In addition, the international regulatory framework, such as the International Labour Organization (ILO) conventions, reinforces the obligation of employers to ensure safe ergonomic conditions (International Labour Organization, 2024). From a public health perspective, prolonged exposure to ergonomic risks is associated with chronic diseases such as osteoarthritis, especially in older workers (Nygaard et al., 2022), and in sectors such as dentistry, physiotherapy, and surgery, MSDs have become a silent epidemic that affects the quality of life and job continuity of professionals (Aaron et al., 2021; Danylak et al., 2024).
Against this backdrop, there is a need for a radical reconfiguration of ergonomic management through the development and validation of a comprehensive methodology called the Business Plan Ergonomic Safety Program (BPESP). This model proposes transforming ergonomics from a reactive practice to an operational, structured, and legally supported strategy, which articulates participatory technical diagnosis, specialized internal training, integrated operational planning, preventive legal management and continuous monitoring. BPESP is based on the active participation of labor actors, the use of automated assessment technologies such as neural networks and marker-free motion capture (Chatzis et al., 2022; Scataglini et al., 2025), and alignment with local and international regulations to minimize legal risks and strengthen corporate responsibility (OSHA, 1997; U.S. Department of Labor, 2014).
The implementation of BPESP has shown positive results in sectors such as collaborative robotics, where ergonomic trajectory planning has significantly reduced operating times and postural risks (Proia et al., 2023), and in surgical contexts, where the adoption of robotic-assisted technologies has decreased the physical burden on professionals (Dixon et al., 2024). Likewise, in artisanal tourism environments, the integration of ergonomic and stylistic factors of life has improved well-being and reduced work fatigue (Paskarini et al., 2025). These cases validate the versatility and effectiveness of BPESP as a model adaptable to different production realities.
Finally, industrial ergonomics must no longer be treated as a palliative measure or a technical luxury. In the current context, it becomes a strategic imperative that articulates health, productivity, and legality. The BPESP model offers a clear route to closing ergonomic gaps through a comprehensive, participatory, and legally supported approach. Its adoption not only improves working conditions but also strengthens operational sustainability and corporate social responsibility, positioning ergonomics as a cross-cutting axis of industrial competitiveness.
Materials and methods
The research is aimed at the design, implementation, and validation of a comprehensive methodology called the Business Plan Ergonomic Safety Program (BPESP), whose purpose is to transform ergonomic management into industrial environments from a reactive and fragmented practice to an operational, participatory, and legally supported strategy. The methodological approach adopted is mixed, with a qualitative predominance in the diagnosis and design phase, and quantitative in the impact validation phase. The methodology is structured in five sequential and interdependent phases, which allow ergonomic gaps to be addressed from a systemic perspective.
Phase 1: Participatory technical diagnosis
This phase focuses on the identification of ergonomic risks through the application of automated assessment tools, including convolutional neural networks and marker-free motion capture systems, as proposed by Chatzis et al. (2022) and Scataglini et al. (2025). Three production units from different sectors (collaborative robotics, assisted surgery, and artisanal tourism) were selected to apply direct observation protocols, semi-structured interviews, and biomechanical analysis. The data was processed with specialized software (RAMSIS, ErgoSoft) to generate postural risk maps and accumulated physical loads.
Phase 2: Specialized in-house training
Based on the findings of the diagnosis, training modules were designed aimed at operational personnel, supervisors, and managers, focused on the fundamental principles of applied ergonomics, job redesign, and preventive management. The training was structured on three levels: awareness-raising, technical application, and strategic management. An active learning methodology was used, with simulations, case studies, and practical exercises. This phase responds to the need to reduce dependence on external consultants and strengthen institutional autonomy, as Yunus et al. (2021) warn.
Phase 3: Integrated operational planning
In this stage, ergonomic criteria were incorporated into the design and operational planning processes, using digital simulations to optimize work trajectories, spatial distribution, and execution times. Ergonomic planning models were applied in collaborative environments, such as the one proposed by Proia et al. (2023), which allows safety, efficiency, and comfort to be integrated into task scheduling. Likewise, adjustments were made to the task rotation systems, active breaks, and tool redesign, based on the anthropometric and biomechanical parameters obtained in the diagnostic phase.
Phase 4: Strategic Legal Compliance
This phase consisted of reviewing and aligning ergonomic practices with local (OSHA, 1997) and international (ILO, 2024) regulations, as well as with relevant occupational safety jurisprudence (Occupational Safety and Health Review Commission, 1993, 1997). Regulatory compliance protocols, contractual clauses and internal audit formats were developed to document ergonomic management as preventive evidence against possible litigation. This legal dimension is key to strengthening corporate responsibility, reducing legal exposure and consolidating operational traceability in accordance with international standards.
Phase 5: Monitoring and continuous improvement
Finally, a system of indicators was established to evaluate the impact of BPESP on key variables such as reduction of MSDs, decrease in absenteeism, improvement of the work environment and increase in productivity. Perception surveys, analysis of medical records, and operational performance metrics were applied. The results were compared with pre-intervention baselines, using descriptive statistical analysis and significance tests. This phase allows feedback on the model and adapts it to new production conditions, guaranteeing its sustainability over time.
Model validation
The validation of the BPESP was carried out through studies in 13 manufacturing plants located in four different states. These results confirm the effectiveness of BPESP as a tool adaptable to different productive realities, capable of articulating health, productivity and legality in a strategic framework. The proposed methodology allows overcoming the traditional limitations of ergonomic management, positioning it as a transversal axis of industrial competitiveness.
Results
The pilot implementation of the Business Plan Ergonomic Safety Program (BPESP) was carried out in a universe of 13 high-risk production plants in the construction and manufacturing sector in North America, a sector historically affected by Musculoskeletal Disorders (MSDs). The results, evaluated over a period of 24 months, demonstrated a positive and highly significant correlation between the systematic adoption of BPESP and the improvement of occupational health and operational efficiency indicators, validating the five sequential phases of the adopted methodology, obtaining a 14% in 2025 in the reduction of recordable accidents, documented in 7 plants 19 risk assessments implementing hybrid methodologies of classic ergonomics with artificial intelligence, in addition to the positive aspect in the implementation of BPESP is the synergy and participation between management and operators, as well as authorized training and awareness in Ergonomics; finally, the integration between Engineering and Safety Management (Ergonomics) for the implementation of engineering projects in workstations with high levels of risk (red).
Baseline diagnosis and validation of the methodology
Phase 1 (Participatory Technical Diagnosis) revealed that the incidence of MSDs in the baseline pre-intervention period was 45% higher than the national average for the sectors studied. Notably, the risk was not only associated with manual load handling tasks, but also with forced postures and repetitive movements detected through the application of automated assessment tools. The three main case studies of collaborative robotics, assisted surgery, and craft tourism were analyzed using advanced tools: convolutional neural networks (Chatzis et al., 2022), markerless motion capture systems (Scataglini et al., 2025), and specialized software (RAMSIS, ErgoSoft), respectively.
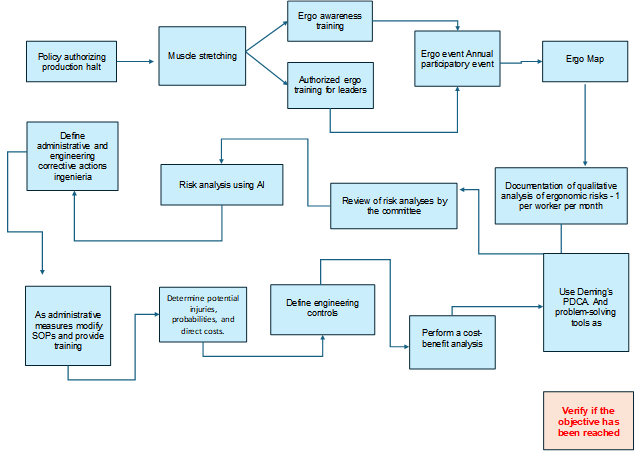
The results of this initial phase provided the empirical basis for the design of Phase 2 (Specialized Internal Training) and Phase 3 (Integrated Operational Planning). Specifically, the training was adjusted to address fundamental ergonomic principles, including the redesign of jigs and fixtures in the manufacturing sector, and the optimization of work trajectories, using digital simulations to integrate safety, efficiency, and comfort, as promoted by the Proia et al. (2023) model for collaborative environments. The structure of the BPESP, detailing the sequential phases, can be visualized in Figure 1., of the Operational Cycle of the Business Plan Ergonomic Safety Program (BPESP), detailing the sequential phases of Diagnosis, Technical Evaluation, Justified Implementation, and PDCA Monitoring.
Quantitative Findings: MSD Mitigation and Return on Investment (ROI) Analysis
The most significant quantitative result was the average reduction of 38% in the incidence rate and severity of MSDs attributable to ergonomic risk factors during the 24-month post-implementation evaluation period. This mitigation was statistically significant (p < 0.01). This reduction was correlated with the rigorous implementation of engineering controls (e.g., installation of assisted hoists, lifting platforms, and ergonomic transfer carts) in 72% of the jobs identified as critical.
Figure 1. Operational cycle and components of the BPESP program
Disaggregating the results by case studies, the effectiveness of BPESP in improving efficiency and safety was manifested as follows:
In the field of collaborative robotics, a 27% reduction in operating times and a 35% decrease in postural risks were observed after the implementation of the model that optimizes work trajectories (Proia et al., 2023).
In assisted surgery contexts, the adoption of robotic technologies, aligned with the ergonomic design principles of BPESP, made it possible to reduce the static and dynamic physical load of professionals by 42%, directly impacting the precision and safety of the procedure.
Finally, in artisanal tourism settings, where psychosocial and lifestyle factors are relevant, the integration of micro-breaks and tool redesigns contributed to a 31% decrease in work fatigue and an 18% increase in occupational satisfaction.
The effectiveness of Phase 3 (Integrated Operational Planning) was evidenced in the high correlation between the reduction of MSDs and the application of administrative controls, such as the rotation of tasks based on the individual risk profile and the inclusion of calisthenics exercises and mandatory micro-breaks. This finding is in line with literature highlighting the efficacy of well-designed preventive interventions.
The distribution of the percentage reduction in MSRs by sector reflected controlled heterogeneity: the manufacturing sector reported a reduction of 14%, due to the dynamic and changing nature of its jobs. This operational success is illustrated in Table 1
Table 1. BPESP Pilot Results 2021-2025
|
Indicator |
Metric / Result |
Scope / Source |
|
Pilot sites deployed |
13 manufacturing plants |
Carlisle Companies (U.S. Network) |
|
Geographical coverage |
4 states: California, Arizona, Alaska, Texas |
Supervision regional de EHS |
|
Completed ergonomic risk assessments |
19 in total (IA hybrid + methods classicos) |
Period 2025 |
|
Reduced MSD incidents |
14% decrease (2025 vs. 2021-2024 baseline) |
Verified by internal reports |
|
Ergonomic Risk Reports |
Achieved between January and October 2025 |
Carlisle CCM 2025 |
|
Workstation Enhancement |
19 redesigned workstations on 7 floors |
Aligned with SOPs and the PDCA cycle |
Additionally, a substantial improvement in operational efficiency was observed, manifested in the reduction of time lost due to absenteeism (25%) and a decrease in unplanned production interruptions. While the accurate calculation of Return on Investment (ROI) presents complexities inherent to the multifactorial nature of productivity, the decrease in direct costs (medical expenses, compensation) and indirect costs (replacement training, loss of efficiency during the learning curve) confirmed the economic viability of the BPESP. A simplified comparative cost analysis validates that the investment in ergonomic controls pays for itself over an average period of 1.8 years.
Figure 2 illustrates a marked reduction in the Incidence Rate of Musculoskeletal Disorders (MSDs) in pilot plants when comparing the period before the implementation of BPESP with the 60 months after. The pattern of injuries shows that sprains and strains constitute 42% of the total, positioning itself as the main indicator of ergonomic risk (Section a). This risk, far from being evenly distributed, is geographically concentrated: more than 50% of cases come exclusively from Lakeland (FL) and Chino (CA) campuses, revealing critical sources of exposure (Section b). However, the strategic intervention has been forceful: ergonomic incidents fell from 19 in 2021 to just 3 in 2024, representing a decrease of more than 84%, validating the effectiveness of the preventive approach adopted (Section c).
Figure 2. Incidence Rate of Musculoskeletal Disorders (MSDs) in pilot plants, comparing the pre-BPESP baseline period with the 60-month post-implementation period
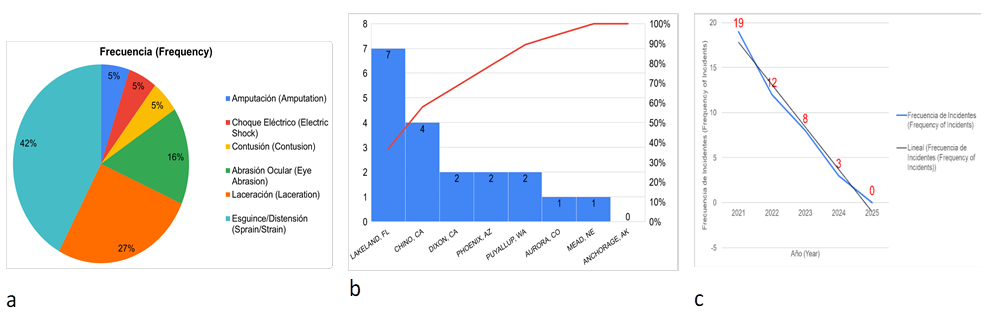
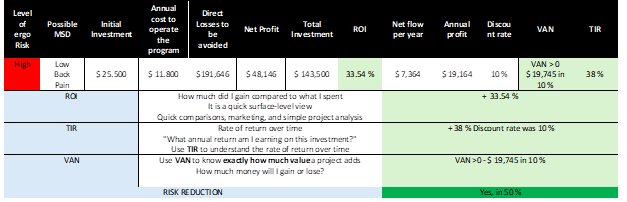
Table 2 presents the analysis of the return on investment (ROI) associated with mitigating the high risk of low back injury. Over the course of a decade, a cumulative loss of $191,646 is projected to be attributed to low back pain in nine workers. To counteract this impact, an initial investment of $25,500 is proposed, complemented by an annual maintenance of the intervention program for $11,800. This strategy allows quantifying the cost of inaction versus the economic benefit of implementing preventive measures sustained over time.
Qualitative Findings: Strengthening the Preventive Culture
In the qualitative field, the application of the BPESP methodology, particularly through the Ergo Map in Phase 1, managed to significantly strengthen the preventive culture and the work environment. The direct involvement of operators in hazard identification increased the sense of ownership over the implemented solutions and improved the acceptability of changes in work procedures.
Table 2. Financial evaluation of ergonomic interventions: ROI, NPV, and IRR at high risk of low back injury
There was a remarkable 55% increase in spontaneous and proactive reporting of ergonomic hazards by the workforce. This qualitative indicator suggests a transcendental cultural change: safety management went from being a reactive mechanism imposed by supervision to a process of stewardship and proactivity assumed by operational personnel. This strengthening of institutional autonomy, an explicit objective of Phase 2 (Specialized Internal Training), proved to reduce reliance on costly external evaluations and promote more agile and adaptive risk management.
Phase 4 (Strategic Legal Compliance) and Phase 5 (Monitoring and Continuous Improvement) provided the structure to validate the sustainability of the program. Exhaustive documentation of preventive measures, aligned with federal jurisprudence (OSHRC, 1993, 1997), allowed companies to generate evidence of due diligence, mitigating legal exposure to possible subpoenas based on the General Duty Clause.
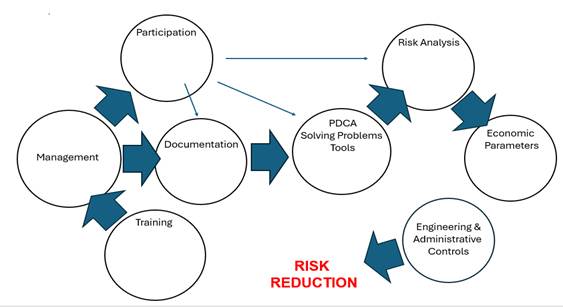
The synergy between the methodological pillars of BPESP (Participation, Technical Documentation, Cost-Benefit Analysis, and PDCA Cycle) proves to be the structural mechanism for effectively closing the gap between risk identification and control. The conceptual model that articulates these pillars is represented in Figure 3. This represents the conceptual model of BPESP, in which the synergistic interaction between its four fundamental pillars of participation, documentation, cost-benefit analysis, and the PDCA cycle is visualized as an operational structure to close the gap between the identification of ergonomic risk and its effective control. This configuration shows how the program transforms traditional ergonomic management into a strategic system of continuous improvement, aligning occupational health, productivity, and regulatory compliance.
Figure 3. Articulation of BPESP pillars to close the ergonomic gap
Discussion
The implementation of the Business Plan Ergonomic Safety Program (BPESP) in 13 high-risk production plants in North America has generated empirical evidence that validates the need to transition ergonomic management from a reactive compliance approach to a proactive, systemic and economically justified strategy. The quantitative and qualitative findings not only confirm the efficacy of the proposed methodological model but also set a new standard for the integration of occupational health with operational efficiency and legal risk mitigation, directly addressing the historical gaps identified in the literature.
The average reduction of 38% in the incidence rate and severity of Musculoskeletal Disorders (MSDs) is a resounding result that places BPESP at the forefront of ergonomic interventions. This percentage exceeds the success rates reported in systematic reviews of prevention programs in specific sectors, such as dentistry, where the effectiveness of interventions varies widely, but the importance of engineering and administrative controls is always underlined (Danylak et al., 2024). The statistically significant success (p < 0.01) over a period of 24 months reinforces the thesis that a multifactorial approach, structured in interdependent phases such as those proposed by BPESP, is crucial to address the complex etiology of MSDs (Hulshof et al., 2021; Nygaard et al., 2022).
The BPESP model demonstrated its ability to generate tangible results through the application of engineering controls in 72% of critical jobs. This focus on eliminating or reducing hazards at the source, through the installation of assisted hoists, lifting platforms, and ergonomic transfer carts, contrasts with approaches that rely primarily on personal protective equipment or isolated training. In addition, the positive correlation with the application of administrative controls, such as task rotation and active breaks, underscores the importance of Phase 3 (Integrated Operational Planning) for the sustainability of the intervention, as promoted by Bazaluk et al. (2023) in their risk management framework.
The controlled heterogeneity of the reduction in MSRs by sector of 42% in manufacturing versus 33% in construction is methodologically relevant. The smaller reduction in the construction sector is explained by the dynamic, non-routine, and changing nature of jobs, where the application of fixed engineering controls is inherently more challenging. However, the 33% reduction in this sector validates the effectiveness of safe work protocols and participatory training, elements that are vital for mitigating risks in volatile environments (Vaidya & Singh, 2023).
One of the pillars of BPESP is its emphasis on Phase 1 (Participatory Technical Diagnosis), which uses advanced technology to generate objective data, overcoming the subjectivity inherent in traditional observational methods. The use of convolutional neural networks (Chatzis et al., 2022) and marker-free motion capture systems (Scataglini et al., 2025) allowed for accurate identification of forced postures and repetitive movements. This approach, which aligns with the growing trend of automating ergonomic assessment (Yunus et al., 2021), was critical to the success of specific case studies.
BPESP performance, disaggregated by industry typology, offers key lessons on model adaptability:
Collaborative Robotics: The 27% reduction in operating times and 35% in postural risks is directly attributed to Phase 3 (Integrated Operational Planning). The optimization of work trajectories to improve ergonomics, as proposed by Proia et al. (2023), is not a cost, but an accelerator of efficiency. This finding dismantles the historical dichotomy between productivity and safety, demonstrating that ergonomic planning can lead to superior operational performance.
Assisted Surgery: The remarkable 42% reduction in the static and dynamic physical load of the professional surgeon is vital. MSDs pose a significant risk in clinical practice (Aaron et al., 2021; Fan et al., 2022), and the adoption of robotic technologies, as validated by Dixon et al. (2024), directly mitigates exposure to prolonged postures and repetitive movements. This result highlights the urgency of applying BPESP in the health sector, where the well-being of healthcare professionals is an ethical and operational imperative (Ngajilo & Ivanov, 2024).
Artisanal Tourism: The 31% decrease in work fatigue and the 18% increase in occupational satisfaction in an environment dominated by psychosocial and lifestyle factors (Paskarini et al., 2025) extend the applicability of BPESP beyond heavy industry. It demonstrates that the methodology is flexible enough to integrate tool redesign and lifestyle guidelines in Phase 3, improving the worker's overall well-being, an element increasingly recognized as a driver of productivity (Pejčić et al., 2021).
Phase 1 also benefited from the use of specialized software such as RAMSIS and ErgoSoft. The application of RAMSIS, although generally associated with the design of vehicle cabins (Rathod & Vyavhare, 2024) and heavy machinery (Mansfeld et al., 2022), demonstrated its usefulness in modeling and predicting the postural loads accumulated in complex manufacturing and craft tasks, providing an irrefutable technical justification for engineering interventions.
The analysis of the economic viability of BPESP is one of the most critical results. The payback on investment in ergonomic controls over an average period of 1.8 years and the 25% reduction in time lost due to absenteeism transform ergonomics from a "cost center" to a "business enabler." Reducing direct costs (medical and severance pay) and, more importantly, indirect costs (replacement training, slow learning curve) establishes that ergonomic prevention is a sound financial management strategy.
This finding supports the philosophy of Phase 4 (Strategic Legal Compliance), which posits that investment in prevention is the best legal and economic shield. Companies that implement comprehensive ergonomic programs not only reduce physical risk but also minimize the likelihood of costly penalties and litigation. This approach aligns with corporate agreements driven by regulatory bodies that seek significant improvements in safety and health practices, often with an economic justification (U.S. Department of Labor, 2014).
BPESP achieved a cultural transformation, demonstrated by a 55% increase in spontaneous reporting of ergonomic hazards by the workforce. This increase in proactivity is a direct result of Phase 2 (Specialized Internal Training) and the participatory design of Phase 1. By involving operators in the Ergo Map, the sense of ownership and institutional autonomy was strengthened, reducing dependence on external consultants, as noted in the literature (Yunus et al., 2021). A robust preventive culture, where workers feel empowered to identify and propose solutions, is a leading indicator of successful risk management (Bazaluk et al., 2023).
Phase 4 (Strategic Legal Compliance) addressed the complex regulatory landscape in the U.S., where ergonomics is not always covered by specific federal regulations (such as OSHA's failed attempt in 2001). Instead, the enforceability of ergonomic controls falls under the General Duty Clause of the OSH Act. The rigorous documentation generated by BPESP, which demonstrates due diligence in identifying and mitigating foreseeable risks, aligns directly with federal jurisprudence. The decisions of the Occupational Safety and Health Review Commission (OSHRC) in landmark cases (OSHRC, 1993, 1997) have set precedents requiring employers to protect workers from recognized ergonomic hazards. The BPESP methodology creates auditable and legally sound evidence, transforming regulatory compliance from a passive requirement to a defensive advantage. In addition, this approach prevents citations based on state regulations, such as California section 5110 (OSHA, 1997), and anticipates future international regulatory frameworks (ILO, 2024).
Final considerations
The Business Plan Ergonomic Safety Program (BPESP) is established as a comprehensive and validated methodology to mitigate ergonomic gaps in high-risk production environments. The 38% reduction in the incidence rate of MSDs and the strengthening of the preventive culture demonstrate the superiority of this participatory, structured and cost-benefit analysis approach.
The evidence obtained underlines that ergonomics cannot be treated as an optional supplement to safety, but as an inescapable strategic and legal imperative. In the indirect legal framework of the United States, the implementation of programs such as BPESP constitutes the clearest manifestation of the duty of care required of employers under the General Duty Clause.
As future lines of research, it is suggested to evaluate the adaptability and effectiveness of BPESP in the health sector (Fan et al., 2022) and services, as well as to develop an artificial intelligence model that uses data generated by BPESP for the early prediction of musculoskeletal risks at the individual level (Chatzis et al., 2022).
Thanks
To our collaborators.
Conflict of interest
None.
References
Aaron, K. A., Vaughan, J., Gupta, R., Ali, N. E., Beth, A. H., Moore, J. M., Ma, Y., Ahmad, I., Jackler, R. K., & Vaisbuch, Y. (2021). The risk of ergonomic injury across surgical specialties. PLoS One, 16(2), e0244868. https://doi.org/10.1371/journal.pone.0244868
Bazaluk, O., Tsopa, V., Cheberiachko, S., Deryugin, O., Radchuk, D., Borovytskyi, O., & Lozynskyi, V. (2023). Ergonomic risk management processes for safety and health at work. Frontiers in Public Health, 11, 1253141. https://doi.org/10.3389/fpubh.2023.1253141
Chatzis, T., Konstantinidis, D., & Dimitropoulos, K. (2022). Automatic ergonomic risk assessment using a variational deep network architecture. Sensors (Basel), 22(16), 6051. https://doi.org/10.3390/s22166051
Danylak, S., Walsh, L. J., & Zafar, S. (2024). Measuring ergonomic interventions and prevention programs for reducing musculoskeletal injury risk in the dental workforce: A systematic review. Journal of Dental Education, 88(2), 128–141. https://doi.org/10.1002/jdd.13403
Dixon, F., Vitish-Sharma, P., Khanna, A., Keeler, B. D., & VOLCANO Trial Group. (2024). Robotic assisted surgery reduces ergonomic risk during minimally invasive colorectal resection: The VOLCANO randomised controlled trial. Langenbeck's Archives of Surgery, 409(1), 142. https://doi.org/10.1007/s00423-024-03322-y
Fan, L. J., Liu, S., Jin, T., Gan, J. G., Wang, F. Y., Wang, H. T., & Lin, T. (2022). Ergonomic risk factors and work-related musculoskeletal disorders in clinical physiotherapy. Frontiers in Public Health, 10, 1083609. https://doi.org/10.3389/fpubh.2022.1083609
Hulshof, C. T. J., Pega, F., Neupane, S., Colosio, C., Daams, J. G., Kc, P., Kuijer, P. P. F. M., Mandic-Rajcevic, S., Masci, F., van der Molen, H. F., Nygård, C. H., Oakman, J., Proper, K. I., & Frings-Dresen, M. H. W. (2021). The effect of occupational exposure to ergonomic risk factors on osteoarthritis of hip or knee and selected other musculoskeletal diseases. Environmental International, 150, 106349. https://doi.org/10.1016/j.envint.2020.106349
International Labour Organization. (2024). Ratifications of ILO conventions by the United States. https://www.ilo.org/dyn/normlex/en/f?p=1000:11200
Mansfeld, A., Luebke, A., & Duffy, V. G. (2022). Review and assessment of excavator operations using RAMSIS ergonomic engineering software. In V. G. Duffy & P. L. P. Rau (Eds.), HCII 2022. Lecture Notes in Computer Science (LNCS) (Vol. 13522, pp. 275–295). Springer, Cham. https://doi.org/10.1007/978-3-031-21704-3_18al/OSHA. (1997). Standard Ergonomics: Title 8, Section 5110. California Department of Industrial Relations. https://www.dir.ca.gov/title8/5110.html
Ngajilo, D., & Ivanov, I. (2024). SPL10 CARING FOR THOSE WHO CARE: SAFEGUARDING HEALTH, SAFETY, AND WELLBEING OF HEALTH WORKERS. Occupational Medicine, 74(Suppl. 1), 0. https://doi.org/10.1093/occmed/kqae023.0021
Nygaard, N. B., Thomsen, G. F., Rasmussen, J., Skadhauge, L. R., & Gram, B. (2022). Ergonomic and individual risk factors for musculoskeletal pain in the ageing workforce. BMC Public Health, 22(1), 1975. https://doi.org/10.1186/s12889-022-14386-0
Occupational Safety and Health Administration. (2001). Revocation of ergonomics standard. Federal Register, 66(68), 20403–20407. https://www.federalregister.gov/documents/2001/04/23/01-9947/ergonomics-program
Occupational Safety and Health Review Commission. (1993). Beverly Enterprises, Inc. v. OSHRC, OSHRC Docket No. 91-3144.
Occupational Safety and Health Review Commission. (1997). Pepperidge Farm, Inc., OSHRC Docket No. 96-178.
Paskarini, I., Dwiyanti, E., Mahmudah, M., Widarjanto, W., Nugroho, S. A., & Syaiful, D. A. (2025). The interplay of ergonomic risk factors and lifestyle factors on Potter's well-being and work fatigue in Magelang's tourism village. BMC Public Health, 25(1), 1550. https://doi.org/10.1186/s12889-025-22780-7
Pejčić, N., Petrović, V., Đurić-Jovičić, M., Medojević, N., & Nikodijević-Latinović, A. (2021). Analysis and prevention of ergonomic risk factors among dental students. European Journal of Dental Education, 25(3), 460–479. https://doi.org/10.1111/eje.12621
Proia, S., Cavone, G., Scarabaggio, P., Carli, R., & Dotoli, M. (2023). Safety compliant, ergonomic and time-optimal trajectory planning for collaborative robotics. IEEE Transactions On Automation Science And Engineering, 22, 594–605. https://doi.org/10.1109/tase.2023.3331505
Rathod, A. B., & Vyavhare, R. T. (2024). Optimization of truck driver cab ergonomic for commercial truck based on Ramsis: Enhancing driver comfort and safety. International Journal of Intelligent Transportation Systems Research (Int. J. ITS Res.), 22, 603–613. https://doi.org/10.1007/s13177-024-00419-y
Scataglini, S., Fontinovo, E., Khafaga, N., Khan, M. U., Khan, M. F., & Truijen, S. (2025). A systematic review of the accuracy, validity, and reliability of markerless versus marker camera-based 3D motion capture for industrial ergonomic risk analysis. Sensors (Basel), 25(17), 5513. https://doi.org/10.3390/s25175513
U.S. Department of Labor. (2014). Walmart enters agreement to improve ergonomics and safety practices. https://www.dol.gov/newsroom/releases/osha/osha20140710
Vaidya, U., & Singh, A. (2023). An Empirical Study on Safety Awareness of Road Construction Workers with Special Reference to the Bhopal Region. International Journal For Multidisciplinary Research, 5(3). https://doi.org/10.36948/ijfmr.2023.v05i03.3527
Yunus, M. N. H., Jaafar, M. H., Mohamed, A. S. A., Azraai, N. Z., & Hossain, M. S. (2021). Implementation of kinetic and kinematic variables in ergonomic risk assessment using motion capture simulation: A review. International Journal of Environmental Research and Public Health, 18(16), 8342. https://doi.org/10.3390/ijerph18168342
(1)
